
Check here every Friday for tips and tricks to help you master Nursing Pharmacology.
Today we are discussing
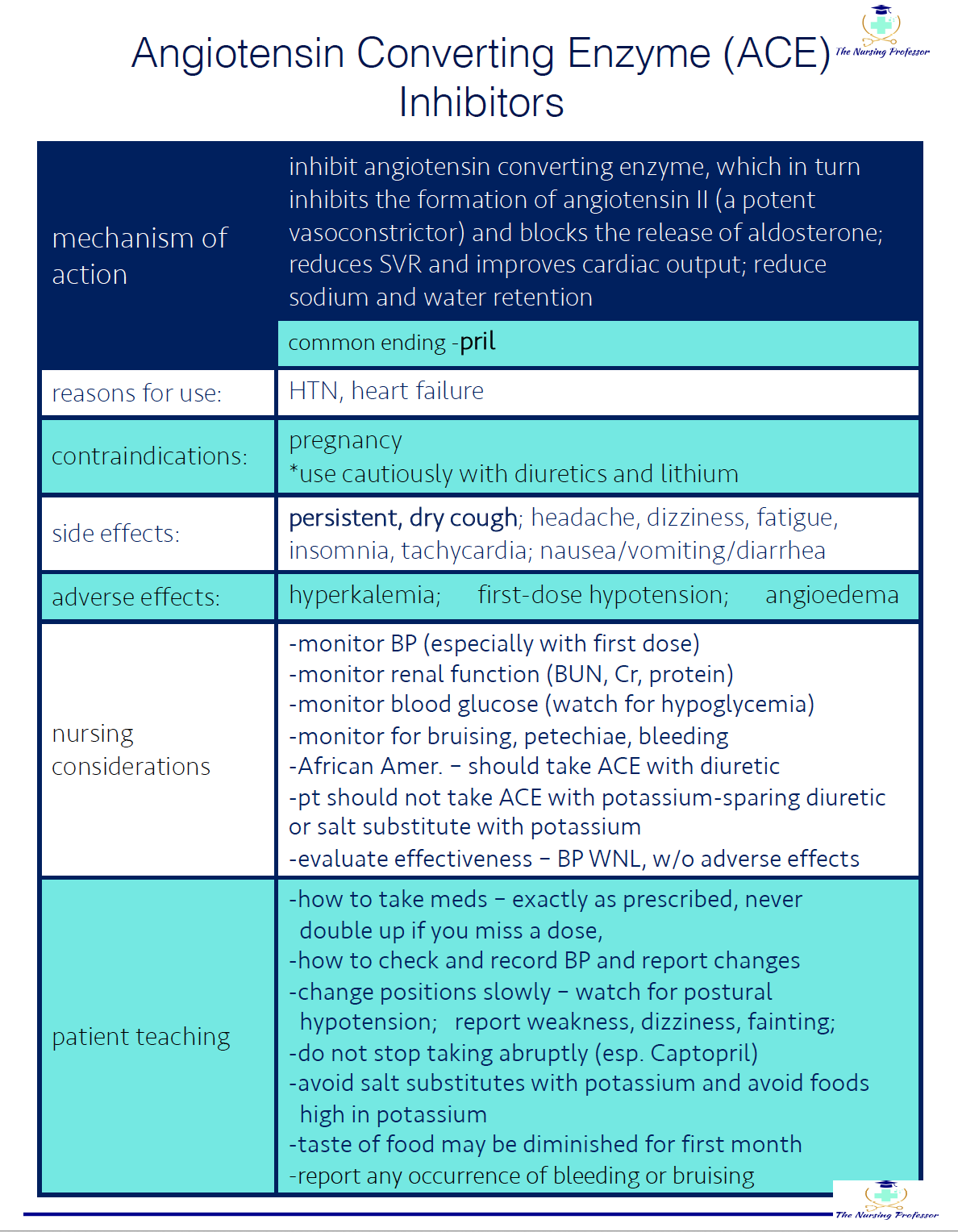
Angiotensin Converting Enzyme (ACE) Inhibitors.
To understand how these meds work, it really helps to ensure you have a good understanding of the Renin-Angiotensin-Aldosterone System (RAAS). I know…not what most students want to hear…but let’s give it a quick review…

Renin-Angiotensin-Aldosterone System (RAAS)
cells near kidney secrete renin
the renin then circulates throughout the body and converts angiotensin into angiotensin I
angiotensin I is converted to angiotensin II in the lungs
angiotensin II, which is a potent vasoconstrictor, then stimulates the adrenal cortex to stimulate test production of aldosterone…
and as a result, the body hangs on to sodium because *ALDOSTERONE SAVES SODIUM* which leads to increased water retention (i.e. circulating blood volume) which increases blood pressure.
So if we are inhibiting angiotensin converting enzyme, then we are preventing angiotensin I from converting into angiotensin II and thereby blocking the release of aldosterone and the sodium and water retention that would coincide with its release. By promoting excretion of sodium and water, ACE inhibitors help to reduce the amount of blood the heart needs to pump and reduces blood pressure.
so…If that’s how they work and what they do, in what instances would they be useful?
Think instances where we need to reduce blood pressure, such as Hypertension (HTN) and Heart Failure (HF).
Other useful info about ACE Inhibitors:
common ending: -pril
examples: benazepril, captopril, enalapril, lisinopril, ramipril
side effects: persistent, dry, hacking cough (*if pt experiences this annoying cough, they should be switched to an Angiotensin Receptor Blocker); headache, fatigue, dizziness, hyperkalemia, tachycardia, orthostatic hypotension
adverse effects: angioedema, bronchospasm
nursing considerations/patient teaching:
teach pt to change positions slowly to avoid orthostatic hypotension
avoid potassium supplements, salt-substitutes, and high-potassium foods
avoid OTC cough meds
notify physician of persistent, dry cough
withhold dose and notify physician if patient develops fever, sore throat, mouth sores, leukopenia, hypotension, or tachycardia
Be sure to check out the cheatsheet and podcast below
Be sure to come back next Friday for another round of Pharmacology Friday!
For pharmacology templates, cheatsheets, practice questions and so much more, be sure to check out our membership, RN School, that has everything you need to Thrive in Nursing School!
